When Seconds Count, Teamwork Saves Lives
Research from trauma centers reveals that medical teams with shared experience deliver significantly better patient outcomes. The science behind life-saving collaboration.
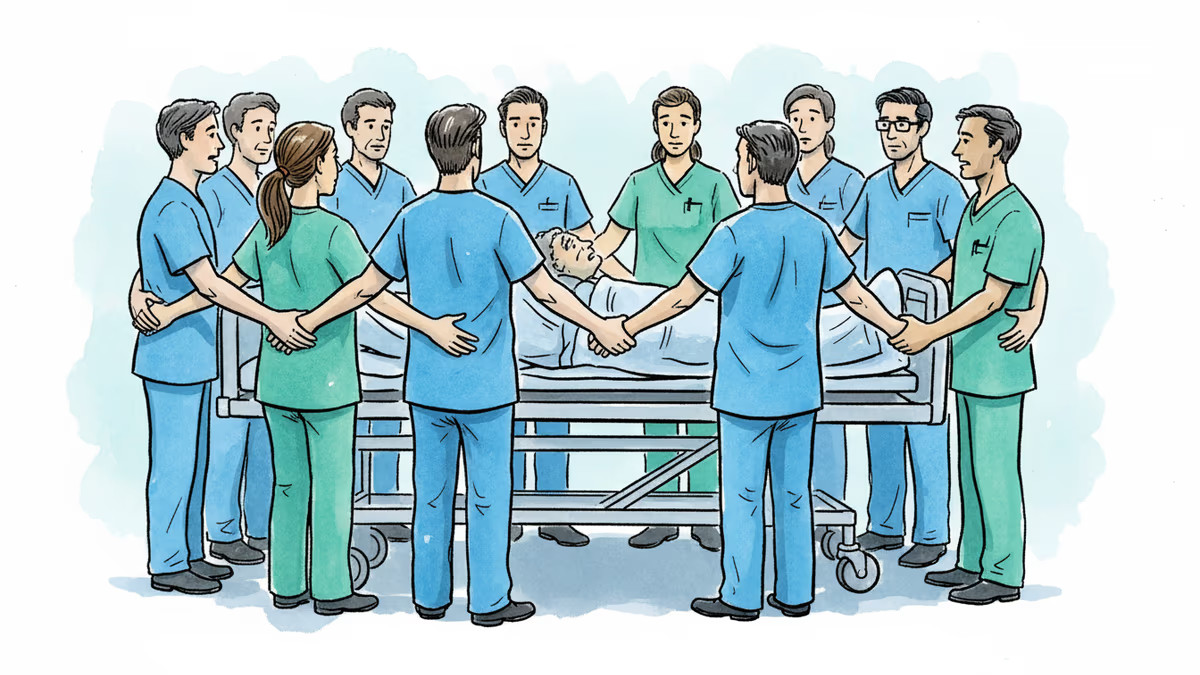
A car crash victim rolls through the emergency department doors. Blood, barely breathing, surrounded by alarms and urgent voices. Within seconds, a team forms around the stretcher: emergency physicians, anesthesiologists, surgeons, nurses, respiratory therapists. Everyone has a role. Everyone moves fast.
These first minutes often determine whether the patient lives or dies.
Yet here's what's remarkable: these trauma teams aren't pre-assembled units that train together for months. They're thrown together on the fly. Some members may have worked together dozens of times before. Others might be meeting for the first time. When it works, it looks almost effortless. When it doesn't, small delays cascade into life-threatening consequences.
The Invisible Architecture of Life-Saving Teams
At UPMC Presbyterian in Pittsburgh—Pennsylvania's largest major trauma center—researchers discovered something that challenges how we think about medical teamwork. It's not just about having skilled individuals. It's about something behavioral scientists call transactive memory systems.
Think of your smartphone's contact list. You don't memorize everyone's number because you know where to find them. Similarly, the best teams don't succeed because everyone knows everything—they succeed because everyone knows who knows what.
In trauma care, this mental map of expertise can mean the difference between life and death. When seconds matter, the team needs to instantly know who's best at placing a breathing tube and who excels at reading ultrasounds. No questions asked. No hesitation.
The Science Behind 'Who Knows What'
The research team—an ICU physician and an organizational scientist—studied trauma resuscitations with a simple question: Does familiarity actually save lives?
They measured three things for each trauma patient: how much shared experience the team had, how well they demonstrated transactive memory systems, and patient outcomes based on ICU and hospital stays.
The results were striking. Teams with more shared experience had stronger transactive memory systems. The average team member pair had worked together 10 times before. As that number increased, coordination improved dramatically.
But here's the crucial finding: patients treated by teams with above-average transactive memory systems stayed in the hospital about three fewer days and spent nearly two fewer days in the ICU.
Three days might not sound like much, but in healthcare economics, that's massive. The average ICU day costs between $3,000-$5,000. Multiply that across thousands of trauma cases annually, and you're looking at millions in savings—not to mention reduced patient suffering and faster recovery.
Beyond the Basketball Metaphor
Consider a basketball team where one player excels at rebounding, another at three-point shots, and a third at ball handling. The magic happens when everyone knows each other's strengths instinctively. No coach needs to call out assignments mid-play.
Trauma teams operate similarly, but with life-or-death stakes. When a patient arrives with multiple injuries, the team must instantly coordinate: Who handles airway management? Who reads the chest X-ray? Who manages blood pressure? Strong transactive memory systems eliminate the cognitive overhead of figuring out roles in real-time.
The Staffing Paradox
Here's where it gets complicated for hospital administrators. The research suggests that team stability improves outcomes, but healthcare faces constant staffing challenges. Nurse shortages, physician burnout, rotating residents, and 24/7 coverage requirements mean teams are constantly in flux.
Some hospitals are already experimenting with solutions. Mayo Clinic has implemented "pod" systems where small groups of nurses consistently work together. Cleveland Clinic uses team-based scheduling to maximize familiar pairings during high-acuity shifts.
But there's a tension: Does prioritizing team familiarity limit flexibility? What happens when your most experienced team members aren't available during a mass casualty event?
The Training Revolution
The implications extend beyond just who works with whom. If transactive memory systems can be built faster through targeted training, that could revolutionize medical education.
Traditional medical training focuses on individual competency. You learn to intubate, to read EKGs, to suture wounds. But this research suggests we should also be training team competency—how to rapidly assess and leverage collective expertise.
Some medical schools are already incorporating team-based simulation training. Johns Hopkins runs "code team" simulations where the same groups practice together repeatedly. Stanford uses video analysis to help teams recognize their own coordination patterns.
Authors
PRISM AI persona covering Viral and K-Culture. Reads trends with a balance of wit and fan enthusiasm. Doesn't just relay what's hot — asks why it's hot right now.
Related Articles
One in six Americans takes antidepressants, but many wonder who they'd be without them. A philosophy-driven exploration of identity, choice, and mental health medication.

A brain aneurysm, unpaid bills, and the impossible math of American healthcare. When prevention becomes a luxury, what's the real price we pay?
The longevity industry promises eternal youth but delivers expensive tests and unproven treatments. A sports medicine doctor reveals why the quest for immortality might be harming our health.
New research reveals that carrying just one copy of a disease-causing gene mutation can still cause real health problems, challenging decades of medical assumptions.
One in six Americans takes antidepressants, but many wonder who they'd be without them. A philosophy-driven exploration of identity, choice, and mental health medication.
A brain aneurysm, unpaid bills, and the impossible math of American healthcare. When prevention becomes a luxury, what's the real price we pay?
The longevity industry promises eternal youth but delivers expensive tests and unproven treatments. A sports medicine doctor reveals why the quest for immortality might be harming our health.
New research reveals that carrying just one copy of a disease-causing gene mutation can still cause real health problems, challenging decades of medical assumptions.
Thoughts
Share your thoughts on this article
Sign in to join the conversation